FMF Certification
Ductus venosus flow
Increased impedance to flow in the fetal ductus venosus at 11-13 weeks’ gestation, is associated fetal aneuploidies, cardiac defects and other adverse pregnancy outcomes. Most studies examining ductus venosus flow have classified the waveforms as normal, when the a-wave observed during atrial contraction is positive, or abnormal, when the a-wave is absent or reversed. The preferred alternative in the estimation of patient-specific risks for pregnancy complications is measurement of the pulsatility index for veins (PIV) as a continuous variable.
Inclusion of ductus venosus blood flow in first-trimester combined screening improves the detection rate for trisomy 21 from about 90% to 95% for a false positive rate of 3%. Assessment of ductus venosus flow need not be carried out in all pregnancies undergoing routine first-trimester combined screening. Such examination could be reserved for the 15% of the total population with an intermediate risk (between 1 in 51 and 1 in 1000) after combined testing.
Requirements for certification
Please attend all online courses through our new FMF website.
From March 2026, registration will be required to qualify for a license extension for the risk calculation software. All new licenses will be issued exclusively through the new website.
To apply for a new license or request a license extension, please follow instructions published on your original FMF Page. Please continue using your original FMF page on this website to apply for and access compatible license files via the Software section.
Note: Some countries have additional certification requirements.
USA: Visit www.fetalmedicineusa.com for accreditation instructions and contact details.
Australia: Contact RANZCOG for accreditation and image submission details.
Further updates and requirements will be posted online soon.
Protocol for images
- The gestational period must be 11 to 13 weeks and six days.
- The examination should be undertaken during fetal quiescence.
- The magnification of the image should be such that the fetal thorax and abdomen occupy the whole image.
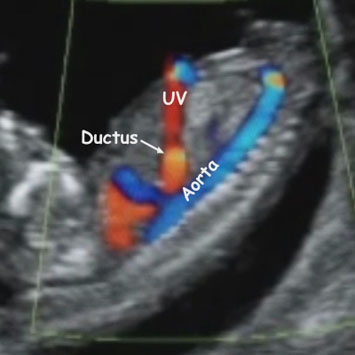
- A right ventral mid-sagittal view of the fetal trunk should be obtained and color flow mapping should be undertaken to demonstrate the umbilical vein, ductus venosus and fetal heart.
- The pulsed Doppler sample volume should be small (0.5-1.0 mm) to avoid contamination from the adjacent veins, and it should be placed in the yellowish aliasing area.
- The insonation angle should be less than 30 degrees.
- The filter should be set at a low frequency (50-70 Hz) so that the a-wave is not obscured.
- The sweep speed should be high (2-3 cm/s) so that the waveforms are spread allowing better assessment of the a-wave.
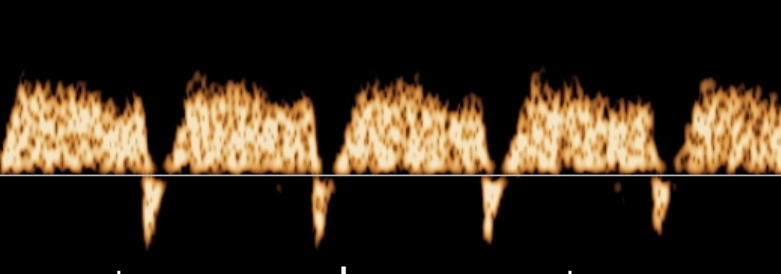
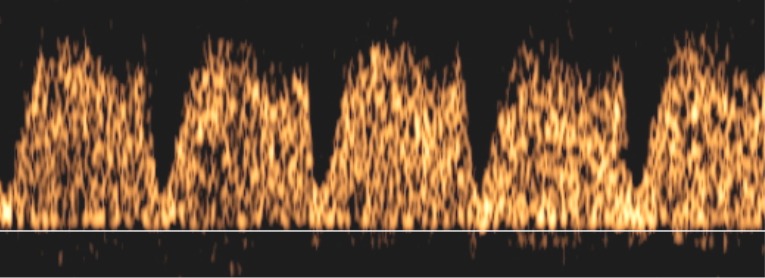
- When these criteria are satisfied, it is possible to assess the a-wave and determine qualitatively whether the flow is positive, absent or reversed.
- The ductus venosus PIV is measured by the machine after manual tracing of the outline of the waveform.
Color Doppler of Ductus venosus
Positive a-wave
Reversed a-wave